Introduction
In the first article of this Practice Management Series, we looked at the big picture: practice management is not just about running the front desk, billing claims, or filling the schedule. It is the operating system that helps a medical practice deliver care reliably, manage complexity, protect revenue, and create a better experience for patients and staff.
In the second article, Patient Access Is Where Practice Management Wins or Breaks, we focused on the front door of the practice. The core idea was simple: patient access is not just scheduling. It is the set of operational steps that determine whether the patient, provider, front office team, and revenue cycle team are ready before care begins.
This third article goes deeper into one of the most important and often frustrating access workflows in U.S. healthcare: prior authorization.
Prior authorization matters because it sits at the intersection of care, coverage, documentation, scheduling, payment, and patient trust. When it works well, care can move forward with confidence. When it breaks, the delay may look like a scheduling problem, a payer problem, a documentation problem, or a billing problem — but the deeper issue is often a coordination problem.
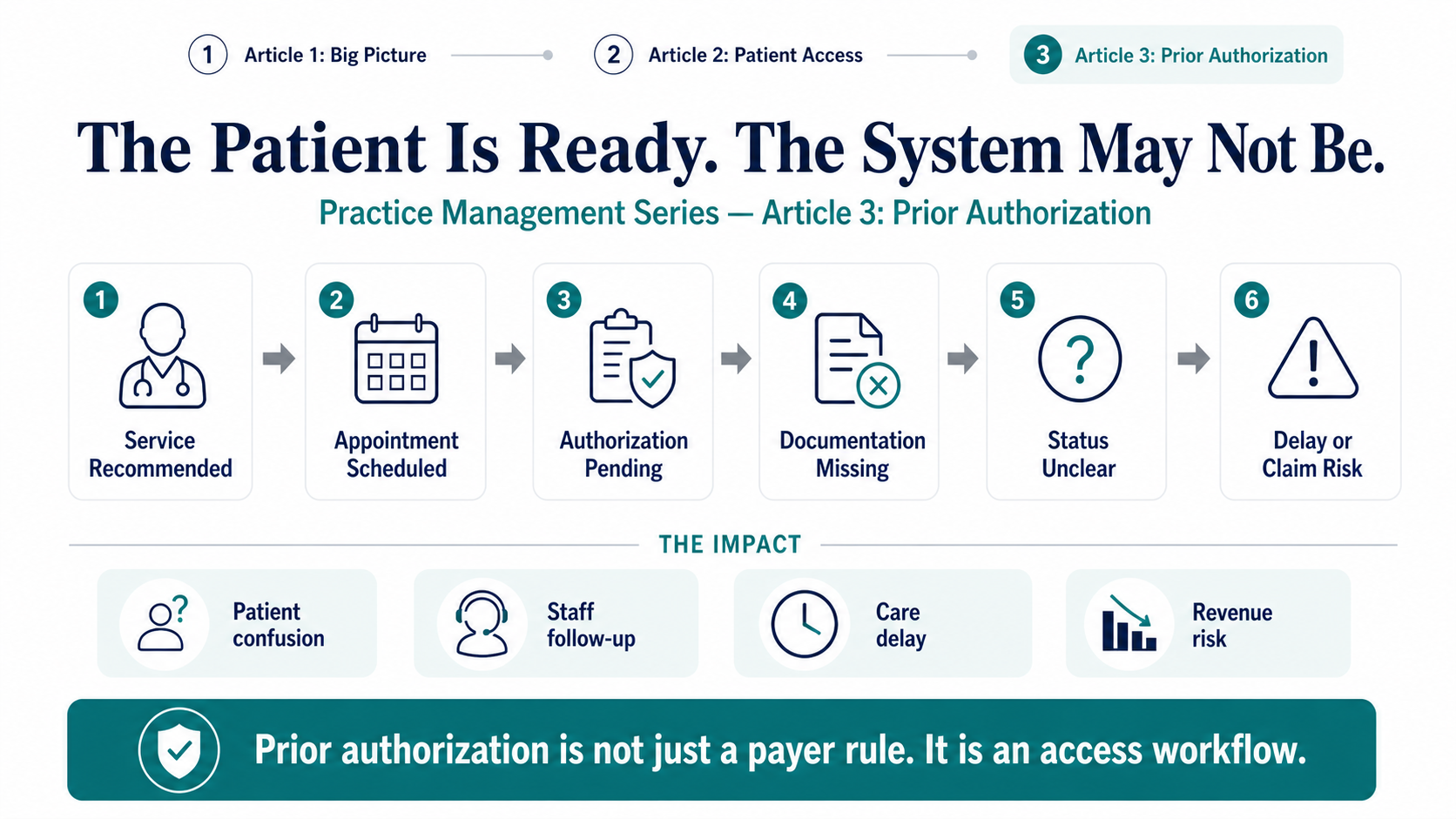
A patient wakes up early for a scheduled MRI. The physician recommended the test. The appointment has been on the calendar for a week. But behind the scenes, the system may not be ready — the imaging center may still be waiting for prior authorization, the payer may require additional clinical notes, and the patient may not know any of this until the day before — or worse, after arriving.
The patient feels confused. The front office feels pressured. The provider's staff must chase status. The imaging center must decide whether to proceed, reschedule, or risk nonpayment. This is the practical reality of prior authorization.
It does not usually fail in one dramatic moment. It fails through a chain of small coordination gaps: unclear requirements, missing documentation, manual follow-up, disconnected systems, and poor visibility into status.
That is why prior authorization should not be understood only as a payer rule. It should be understood as an access workflow. And when that workflow is manual, fragmented, or opaque, care does not move forward with confidence.
What Prior Authorization Is — and What It Is Not
Prior authorization is approval from a health plan that may be required before a patient receives a service, procedure, medication, device, test, admission, or treatment in order for it to be covered by the plan. CMS explains the timing clearly: under prior authorization, the provider or supplier submits the request and receives the decision before services are rendered.
That timing is what makes prior authorization so important to practice management. It happens before care. It happens before the claim. It happens before payment. And often, it happens before the patient fully understands what is still missing.
In practice, prior authorization asks a set of administrative questions:
Is this patient covered?
Is this service included in the patient's benefit?
Is this provider or facility allowed under the plan?
Is the requested service medically necessary under the payer's policy?
Is the required documentation complete?
Do the timing, site of care, code, diagnosis, and requested units align with the rules?
That makes prior authorization more than a form. It is a decision workflow.
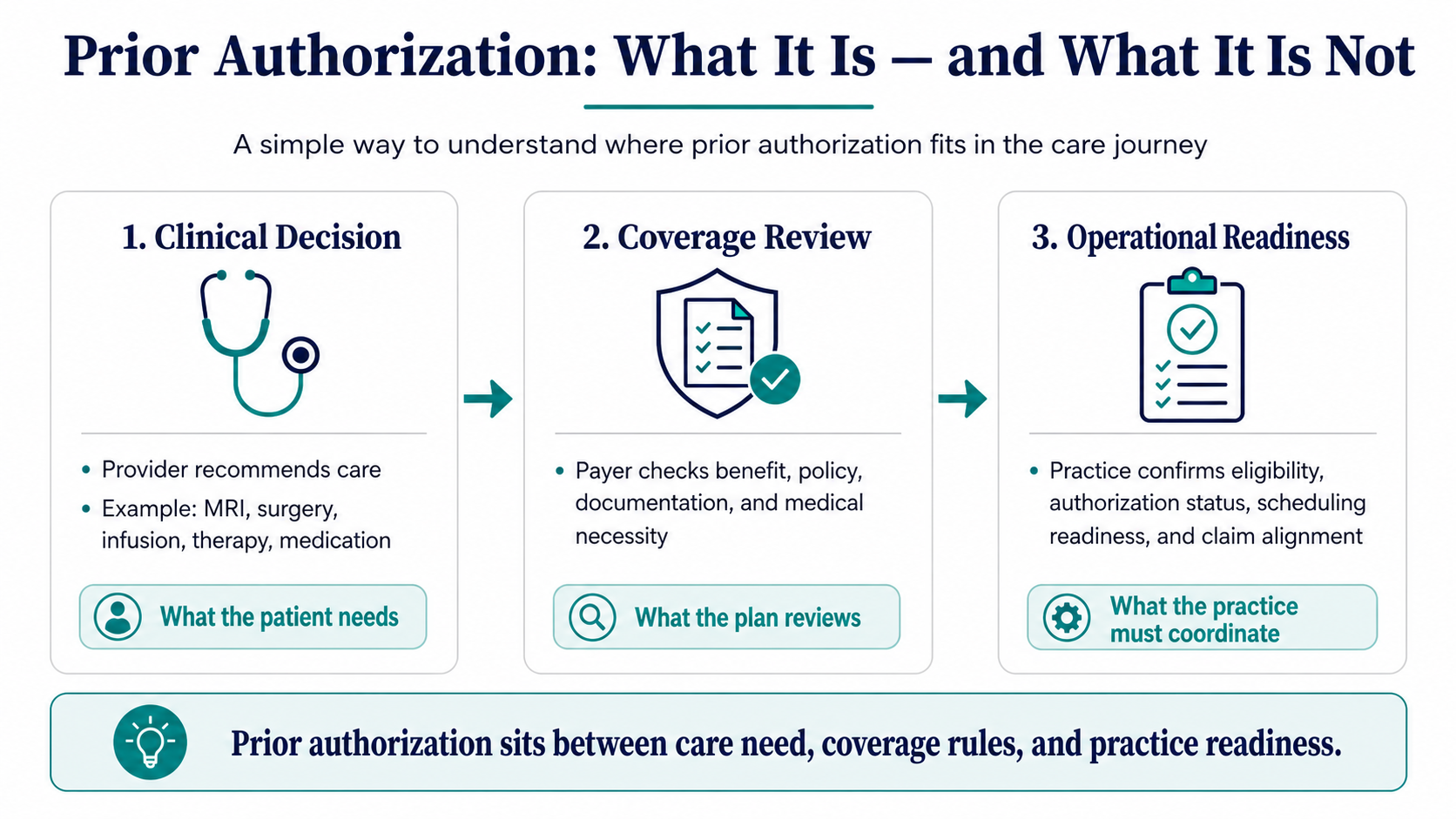
It is also important to clarify what prior authorization is not. It is not the same as the doctor's clinical decision. A physician may decide that a patient needs an MRI, surgery, infusion, therapy, or specialty medication — that is a clinical decision. Prior authorization asks a different question: will the payer, plan, or administrator approve coverage for that service under the patient's benefit and policy rules before the service happens?
It is also not a guarantee of payment. Even when authorization is approved, the final claim must still match the approved terms: patient, provider, facility, service code, diagnosis, date range, units, place of service, and other plan rules. If those details do not match, the claim may still be delayed, reduced, or denied.
Clinical decision: the provider believes the patient needs care.
Coverage review: the payer determines whether the requested care meets coverage, benefit, and policy requirements.
Operational readiness: the practice determines whether the patient, appointment, documentation, authorization, and billing handoff are ready before the service happens.
Most prior authorization pain comes from the gap between these three decisions. The clinician may be ready. The patient may be ready. The appointment may be scheduled. But the coverage and operational readiness may still be incomplete. That is why a scheduled appointment is not enough.
Why Prior Authorization Exists
Prior authorization did not begin as a patient-experience workflow. It began as a utilization management tool.
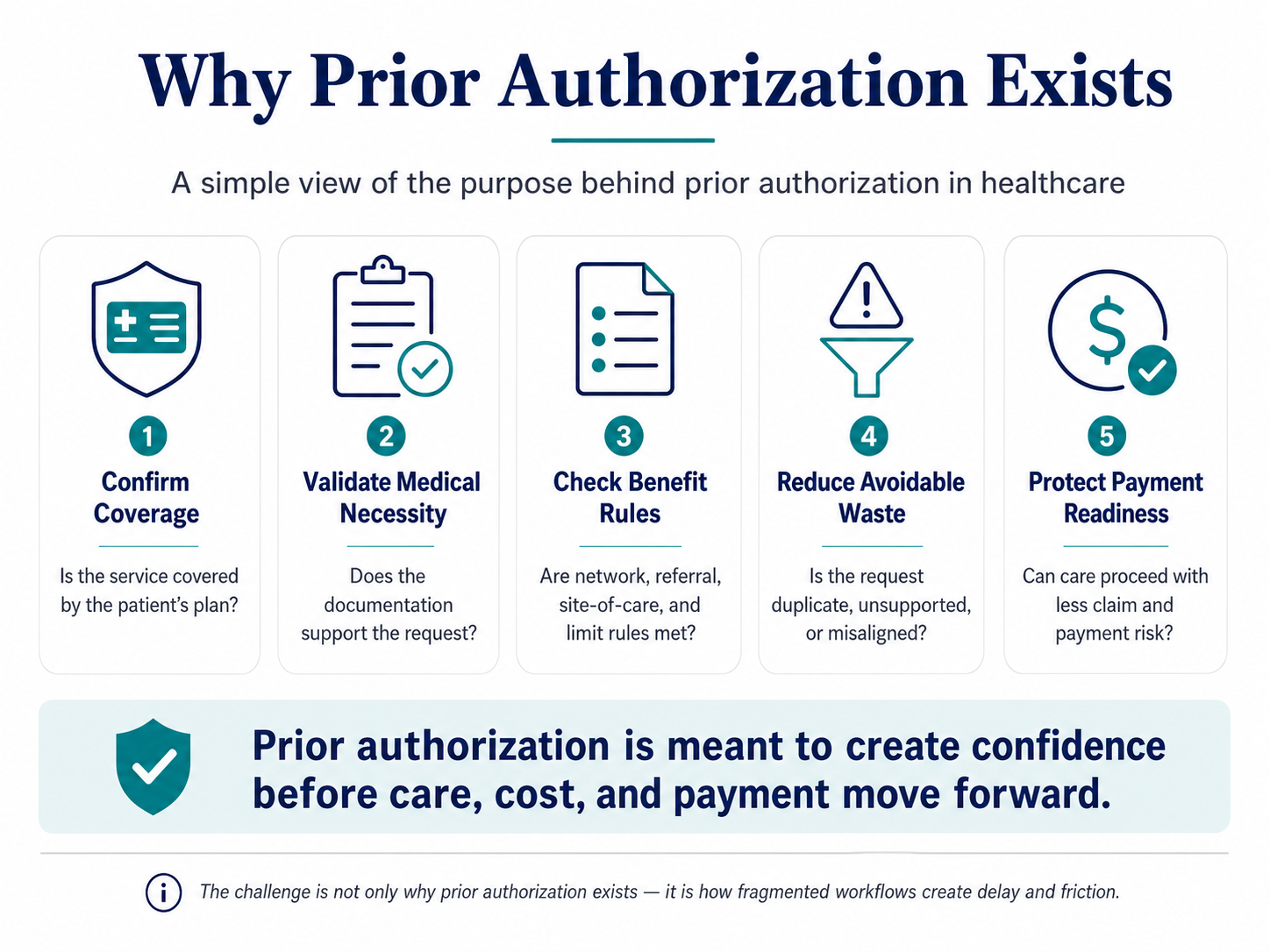
At its best, prior authorization is intended to confirm that a requested service is covered, medically necessary, safe, appropriate, and aligned with the patient's plan rules before the service is delivered. That purpose matters. A balanced discussion should not treat prior authorization as simply "bad." It has legitimate goals: confirming coverage, validating medical necessity, protecting benefit rules, reducing avoidable waste, and managing cost.
For example, a payer may require documentation before approving an MRI for back pain. A plan may require step therapy before a specialty medication. A surgery may require review to confirm diagnosis, procedure code, provider, facility, and site of care. Home health or durable medical equipment may require documentation that supports medical necessity.
In each case, the payer is not simply asking, "Did a doctor order it?" The payer is asking, "Does this request meet the coverage and policy rules for this patient's plan before the service occurs?"
That distinction is important because it explains why the workflow becomes so complex. The provider has the clinical rationale. The payer has the policy rules. The patient has the need. The practice has the appointment. The facility has the service location. The revenue cycle team has the future claim risk. The documentation may be scattered across notes, referrals, labs, images, forms, and portals.
Prior authorization exists because someone must reconcile all of that before care moves forward. The problem is not only the review. The problem is the coordination burden.
Prior authorization has a legitimate purpose, but the workflow needs better infrastructure.
When Prior Authorization Is Triggered
Prior authorization is triggered when a health plan requires approval before a service, medication, device, procedure, test, admission, or treatment is delivered or covered. The trigger usually happens before the appointment, procedure, prescription fill, admission, or service delivery. But in many practices, the need for authorization is discovered too late — after the patient is already scheduled, after the provider has ordered the service, or after staff have started coordinating the visit.
That is why prior authorization should be treated as an access-readiness checkpoint, not a back-office task. Before an authorization-sensitive service moves forward, the practice needs to know:
Is the patient covered?
Is the service covered?
Is prior authorization required?
What documentation is needed?
Do the provider, facility, code, diagnosis, date, and units match the plan rules?
Can the patient proceed with confidence?
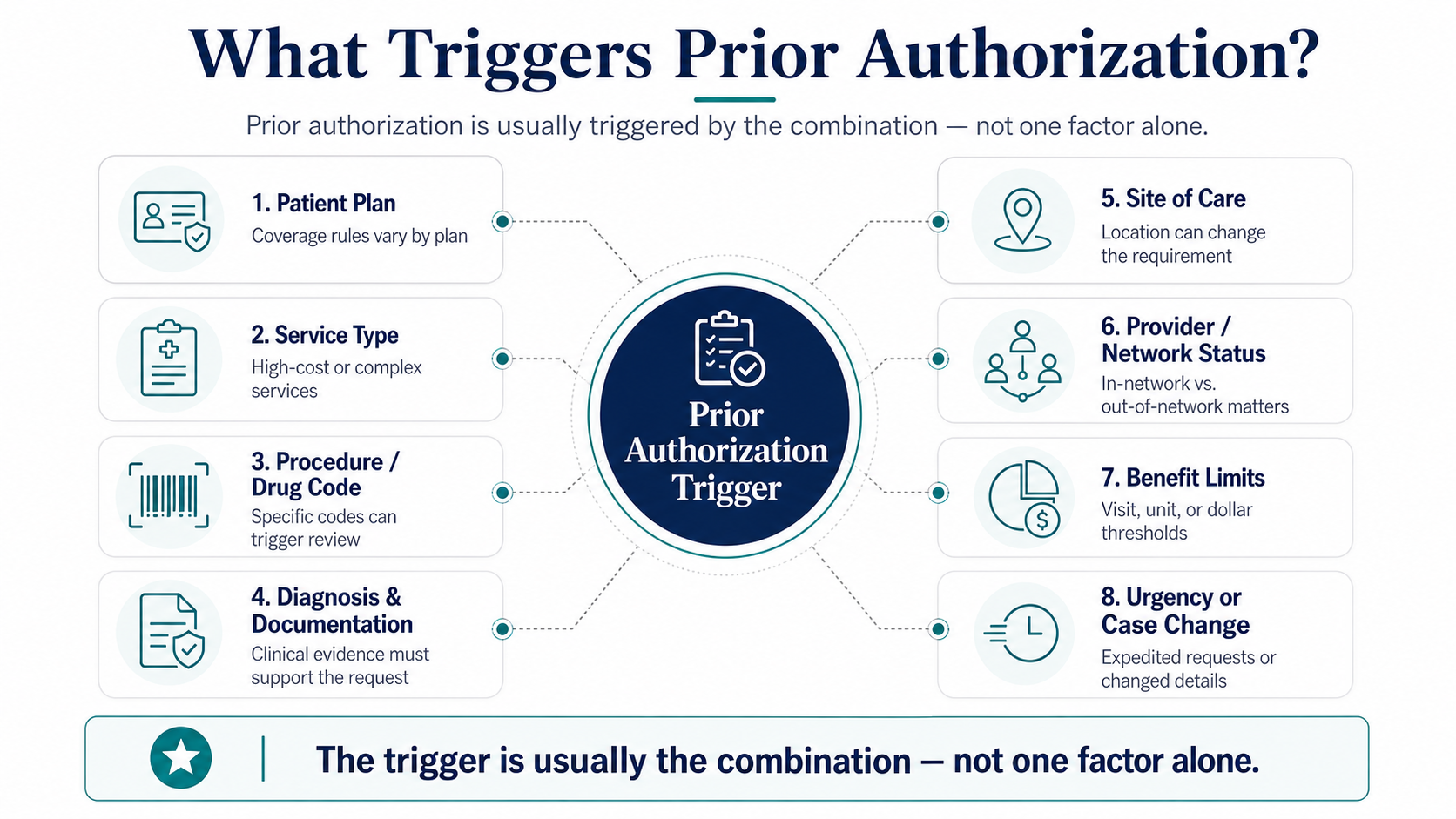
Prior authorization is rarely triggered by one factor alone. It usually depends on the relationship between the patient, plan, service, documentation, provider, and setting. The most common triggers include:
The patient's plan requires it
Requirements vary across commercial plans, Medicare Advantage plans, Medicaid managed care plans, employer-sponsored plans, pharmacy benefit programs, and self-funded employer arrangements.
The service is high-cost or high-risk
Common examples include advanced imaging, elective surgeries, specialty drugs, infusions, durable medical equipment, home health, skilled nursing, inpatient rehabilitation, and behavioral health higher levels of care.
The code triggers review
Authorization rules are often tied to CPT, HCPCS, revenue, diagnosis, drug, or place-of-service codes. If the practice checks authorization using a general description but the actual code changes later, the authorization may not match the claim.
The diagnosis and documentation must support the request
A payer may require symptom history, test results, prior treatment history, conservative therapy documentation, lab values, or evidence of treatment failure.
The site of care changes the requirement
The same service may be treated differently in a physician office, imaging center, hospital outpatient department, ambulatory surgery center, inpatient setting, pharmacy, home, or infusion center.
Limits, urgency, or case changes
Additional therapy visits, extended home health, additional inpatient days, post-acute care extensions, changed service dates, or insurance changes can create new authorization requirements.
Prior authorization is triggered by the relationship between the patient, plan, service, documentation, provider, and setting — not by one factor alone.
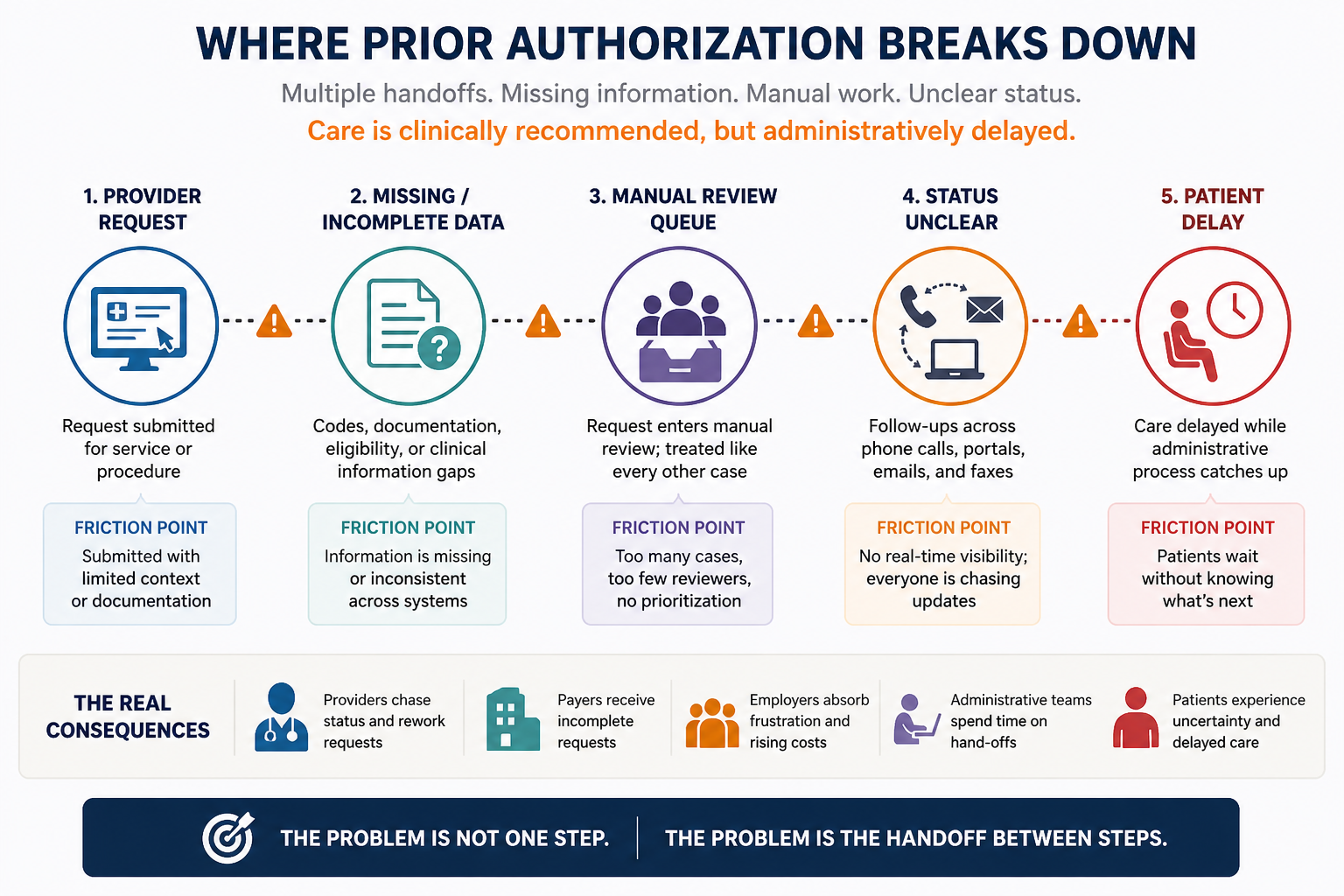
Why Prior Authorization Breaks Down
Prior authorization does not usually fail because one person forgot to do their job. It breaks down because the process depends on too many disconnected steps.
A provider may need to confirm eligibility. A payer may need the right diagnosis, procedure code, and documentation. A patient may be waiting without knowing what is missing. A scheduler may not know whether the appointment is safe to confirm. A revenue cycle team may later discover that the claim does not match the authorization.
Care is clinically recommended, but administratively delayed.
Prior authorization is not just a form. It is a coordination workflow across multiple organizations. When each organization uses different systems, rules, timelines, and communication channels, delay becomes the default.
Common breakdowns include:
Requirements discovered too late.
Clinical documentation missing or incomplete.
Codes changing after authorization discovery.
Payer portals requiring manual rekeying.
Status trapped in phone calls, faxes, emails, or portals.
Every request treated like an exception.
Patients forced to chase updates between organizations.
Approved authorizations failing to match the final claim.
The opportunity is not simply to "speed up paperwork." The opportunity is to redesign prior authorization as a coordinated decision flow — where the right information is captured earlier, rules are applied consistently, missing items are surfaced quickly, and humans focus on exceptions instead of every routine case.
The problem is not one step. The problem is the handoff between steps.
The End-to-End Prior Authorization Workflow
Prior authorization is often described as a single task: "Get the auth." But in reality, it is a sequence of decisions, validations, handoffs, and status updates that must happen before care can move forward with confidence.
A practical end-to-end workflow looks like this:
Prior authorization is not complete when the request is submitted. It is complete only when the decision is clear, the appointment is ready, and the downstream claim can match the approval.
This is where practices often underestimate the workflow. Submission feels like progress, but submission is not completion. A request may be submitted but missing documentation. It may be approved but for the wrong facility. It may be valid but expire before the appointment. It may authorize fewer units than the treatment plan requires. It may approve one code while the claim is submitted under another.
That is why prior authorization should connect all the way from order to claim. The goal is not just to get approval. The goal is to create a clean, traceable path from clinical recommendation → administrative readiness → care delivery → payment clarity.
What the Data Shows
The prior authorization burden is not just anecdotal. Patients feel it as delay. Providers feel it as administrative work. Payers feel it as review volume. Practices feel it as staffing pressure, rework, and revenue-cycle risk.
How large is the volume?
In Medicare Advantage alone, KFF reported that insurers made nearly 53 million prior authorization determinations in 2024, up from 49.8 million in 2023. KFF also reported that 4.1 million requests, or 7.7%, were denied in full or in part. Only 11.5% of denied requests were appealed, but 80.7% of appealed denials were overturned.
What does the AMA report?
The AMA's 2024 physician survey reports that prior authorization creates substantial administrative burdens for physicians and staff, takes time away from direct patient care, costs practices money, and contributes to physician burnout.
What is the savings opportunity?
CAQH's 2024 Index estimates that adopting the electronic standard for prior authorization could save the industry $515 million annually and save medical providers and staff 14 minutes per authorization.
What is the regulatory direction?
CMS's Interoperability and Prior Authorization Final Rule requires impacted payers to implement a Prior Authorization API that can identify covered items and services, documentation requirements, and support prior authorization requests and responses. Prior authorization is moving from a phone-and-fax workflow toward a digital, measurable, interoperable infrastructure problem.
If prior authorization is becoming more digital and measurable, is the practice operating model ready?
A practice does not need to solve the entire healthcare system. But it does need a better way to manage its own authorization-heavy workflows. That means knowing: which services generate the most authorization work, which payers create the most rework, which requests are delayed because documentation is missing, which cases are stuck in pending status, which approvals fail to match the final claim, how much staff time is spent chasing information, and how often patient care is delayed because the next step is unclear.
These are not just operational details. They are management signals. If a practice cannot see the authorization workflow, it cannot improve it.
The InfraHealth Perspective
From the InfraHealth perspective, prior authorization is exactly the kind of workflow that reveals why healthcare needs better coordination infrastructure. The issue is not only that prior authorization exists. The issue is that too much of it still depends on manual discovery, fragmented portals, unclear status, repeated follow-up, and disconnected handoffs between care, coverage, scheduling, and payment.
Eliminate administrative friction so access to quality healthcare is fast, universal, and inevitable.
Prior authorization is a powerful place to begin because it directly blocks access to care, is highly administrative, is measurable, and has clear automation potential. This is primarily an external friction problem because it crosses providers, payers, patients, employers, benefit administrators, facilities, and technology systems.
A better prior authorization operating model should:
Detect requirements earlier.
Collect the right documentation upfront.
Use existing systems and standards wherever possible.
Show status and ownership clearly.
Route routine cases faster.
Escalate complex cases to humans.
Connect authorization decisions to scheduling and claims.
This preserves human oversight while reducing unnecessary waiting. The goal is not automatic approval. The goal is faster clarity, fewer avoidable delays, and better confidence before care moves forward.
Closing Thought
Prior authorization will not disappear overnight. It has legitimate purposes: confirming coverage, validating medical necessity, protecting benefit rules, and managing cost. But the current operating model often creates too much avoidable friction for patients, providers, payers, employers, and practice teams.
The path forward is not more manual follow-up. The path forward is better infrastructure.
Prior authorization should not depend on who calls the payer the most, who remembers to check the portal, or who escalates the loudest. It should move forward because the workflow is visible, the requirements are clear, the missing information is known, and the next step is assigned.
That is the real opportunity. And it is why prior authorization is one of the best places to begin if we want to improve practice management, reduce administrative burden, and accelerate access to care.
Talk to InfraHealth ->